During the fall, I served as the lead client researcher for the Digital Legacy Clinic, a startup that focuses on providing support for end of life digital planning and post-mortem platform support. Our goal was to build partnerships with local organizations such as hospices, retirement homes, and death doulas who could refer clients to us. Because partnering with outside institutions was new for our clinic, I needed to build a process from the ground up that helped us understand each type of organization, what they were capable of taking on, and where our services might naturally support their existing work.
Overview
Research and Scoping
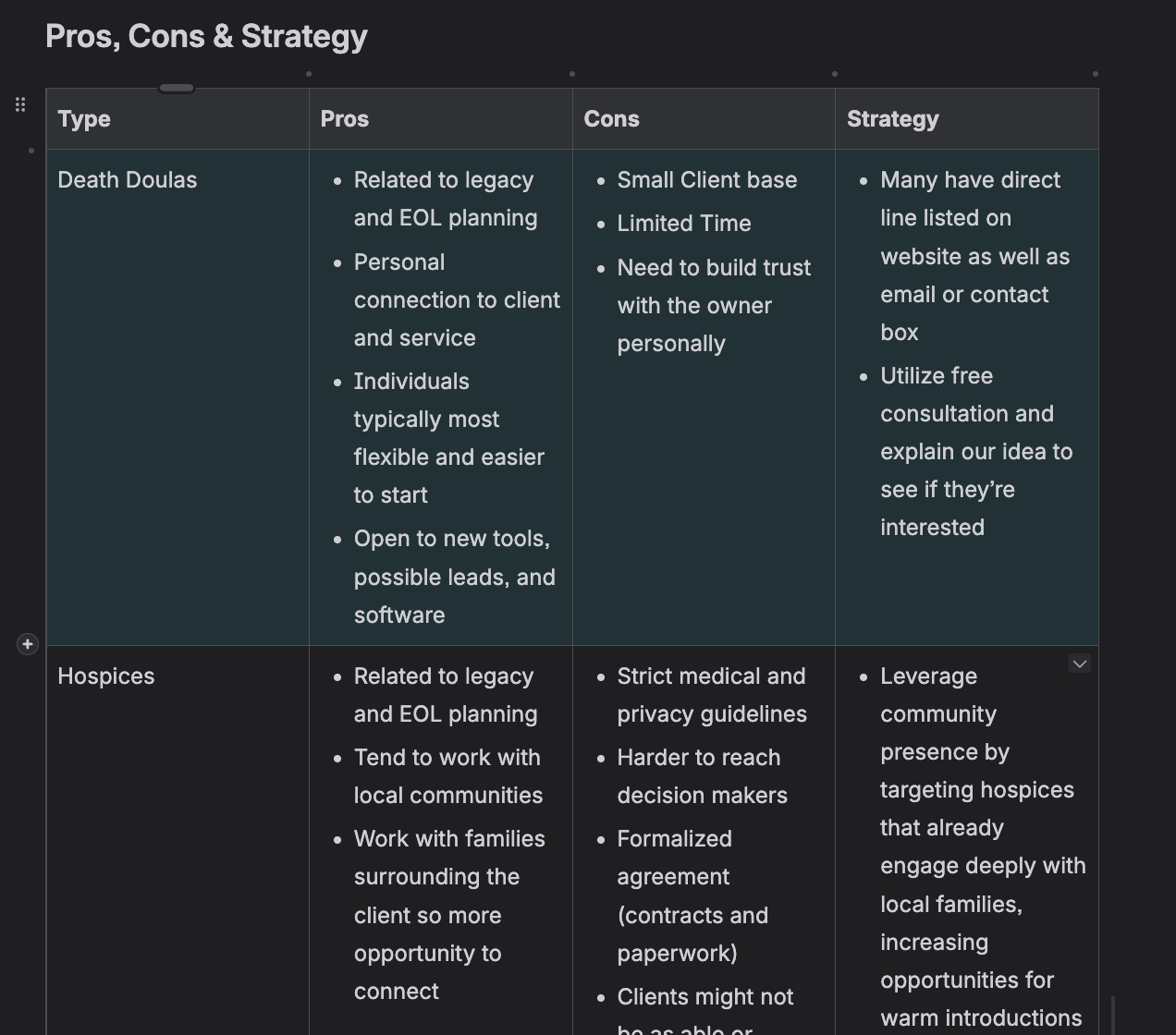
Early on, it became clear that each of these institutions operates very differently, so before we reached out to anyone, I focused on mapping out their structures, abilities, and constraints. Retirement homes typically had established activity or support programs with dedicated staff, hospices operated under much tighter medical and legal protocols, and death doulas worked more independently with highly personal, case by case relationships. Documenting these distinctions helped set realistic expectations for what a partnership might look like in each setting. I then met regularly with our central client communications team to compare what I was learning with their ideal client flow. These discussions helped us figure out which organizations would be the best initial fit and which would need longer term nurturing before anything formal could be established. This shared understanding across teams became essential for keeping our outreach grounded and consistent.
Outreach Strategies
Once the research felt clear, I compiled a list of twenty potential partners: ten retirement homes, five hospices, and five death doulas. From there, I created flexible email templates tailored to each group. The goal was not to standardize our communication but to reduce the initial friction so that every outreach message was consistent in tone while still leaving plenty of room to personalize it based on the organization’s mission, values, and community.
Our team decided early on that we did not want these conversations to feel like sales pitches. Instead, we approached each outreach as an informational conversation and an opportunity to understand what these institutions were already doing, where they felt they had gaps, and how our clinic might be able to support them without adding any unnecessary strain.

As we moved further into outreach, we experimented with different communication methods: in person visits, emailing, and calling. Throughout this process, we took detailed notes on what worked, what did not, and why. Surprisingly, we found that in person visits, even when they were cold calls, worked far better than we expected. Staff responded well to the fact that we were genuinely trying to learn about their work rather than simply asking them to send clients our way. That intention carried through in our conversations and helped us begin these relationships on the right foot.
Challenges
One of the biggest challenges was the real possibility that we might not secure any partnerships at all. We did not want to assume that we were entitled to these relationships, so we focused heavily on building a sustainable process rather than centering the project around a specific outcome. That way, even if we failed to acquire partnerships, future clinic members would have clear documentation on what approaches had been tried and where the sticking points were.
Another challenge came later when we began thinking about sustainability. Many of us would not be continuing with the clinic next semester, and these relationships were still new and somewhat fragile. To prevent the partnerships from collapsing as soon as we left, we put the organizations in direct contact with the clinic’s director and drafted email templates that would help new members maintain communication without having to start from scratch. We also wrote detailed documentation on each organization including how they preferred to communicate, what they valued most, what concerns they raised, and what stage of partnership we had reached with them. This allowed next semester’s team to inherit a clear roadmap rather than a list of disconnected leads.
Outcomes
Our emphasis on trust and relationship building shaped the success of our outreach. By approaching organizations with curiosity and a genuine interest in their work, we were able to begin these conversations on strong footing. Over the course of the semester, we confirmed two formal partnerships, and several additional organizations remained in ongoing discussions with us. These were not superficial commitments. Each group expressed genuine interest in collaborating, and the discussions were grounded in what they actually needed rather than what we hoped they would want.

Beyond the partnerships themselves, the most significant outcome was the foundation we created for the clinic. We now have a researched understanding of the local ecosystem of end of life organizations and a structured outreach process that future teams can use and adapt. We documented communication strategies, common concerns, and the reasons certain outreach methods worked better than others. As a result, even organizations that did not formally partner with us still left the conversation with a stronger awareness of the clinic’s purpose and might end up referring clients to us informally over time.
Establishing this groundwork means the clinic now has a clearer path forward for growth. The partnerships we formed, along with the ones still in progress, feel like the beginning of something sustainable rather than a one semester effort that will disappear once the team changes.
Reflection
Working on this project taught me how important it is to lead with curiosity rather than persuasion when building partnerships. The most productive conversations happened when I focused on understanding the institution first, including its pressures, boundaries, and staff capacity, and then explored how our clinic might be able to help. Approaching the work in this way made the conversations feel more collaborative and less like we were trying to convince anyone of anything.
Coordination across teams was also essential. Translating my research into something that matched our client communications workflow required regular communication and a willingness to revise our strategy as we learned more. This experience reinforced how relationship building is almost always a slow process, and that careful documentation and continuity planning matter just as much as the initial outreach.
Overall, this project strengthened my understanding of partnership development as a form of long term community building. It gave me a much deeper appreciation for the kinds of institutions surrounding end of life care and how the Digital Legacy Clinic can fit into that ecosystem in a way that is respectful, helpful, and sustainable. It also reminded me that leadership in this kind of work often means creating clarity for the team, setting realistic expectations, and preparing the groundwork so that others can step in and continue the effort without losing momentum.